Imagine a pain so intense that it has been called the "suicide disease" — a condition where even the lightest touch to the face, a gentle breeze, or the simple act of brushing one's teeth can trigger an electric shock-like sensation of agony. This is the daily reality for millions of people worldwide living with trigeminal neuralgia (TN), a chronic pain disorder affecting the trigeminal nerve — the fifth and largest cranial nerve in the human body.
For decades, the standard treatment ladder has been medication (with diminishing returns and mounting side effects) followed by invasive surgical procedures that carry significant risks. But at Guangzhou Concord Cancer Center (GCCC), an advanced non-invasive solution is changing the equation: Gamma Knife radiosurgery.
What Is Trigeminal Neuralgia?
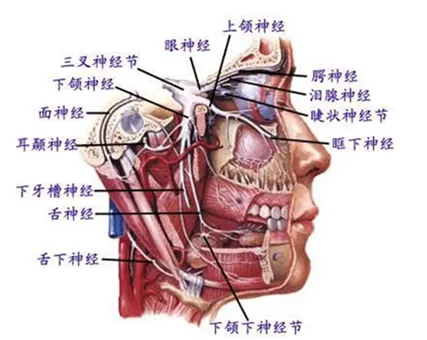
Trigeminal neuralgia — known historically as tic douloureux — is a chronic pain condition affecting the trigeminal nerve, which carries sensation from the face to the brain. The nerve divides into three branches:
- Ophthalmic branch (V1) — forehead, upper eyelid, and scalp
- Maxillary branch (V2) — lower eyelid, cheek, nostril, upper lip, and upper gum
- Mandibular branch (V3) — lower lip, lower gum, jaw, and muscles of mastication

Trigeminal neuralgia predominantly affects middle-aged and elderly populations, with a female-to-male ratio of approximately 3:2 and an average onset age of 53 to 57 years.
Globally, the annual incidence of trigeminal neuralgia is approximately 4 to 5 per 100,000 people, making it one of the most severe forms of neuropathic pain known to medicine. The pain attacks are characteristically sudden, severe, and brief — described by patients as feeling like electric shocks, stabbing, or burning sensations that last from a few seconds to several minutes.
What makes this disease especially cruel is the presence of trigger zones — small areas around the mouth, nose, or cheek where even the lightest stimulation can provoke a full-blown attack. Over time, patients begin avoiding essential daily activities like eating, drinking, speaking, and oral hygiene for fear of triggering pain. In advanced cases, severe depression and suicidal ideation are not uncommon.
The Four Treatment Pathways: A Comparison
1. Medication (First-Line, But Not a Cure)
The first line of defense typically involves anticonvulsant medications such as carbamazepine, oxcarbazepine, gabapentin, and pregabalin. These drugs work by suppressing electrical discharges within the trigeminal nerve. However, medication cannot cure trigeminal neuralgia — it only manages symptoms. As the disease progresses, higher doses are required, leading to escalating side effects including dizziness, fatigue, liver toxicity, and cognitive impairment. Drug resistance eventually develops in many patients.
2. Nerve Ablation (Destructive Procedures)
Techniques including radiofrequency thermocoagulation, glycerol injection, and balloon compression of the trigeminal ganglion deliberately destroy nerve fibers to block pain signals. While effective in the short term, these procedures carry risks of permanent facial numbness, sensory loss, corneal anesthesia, and jaw weakness. The procedure itself can be painful, and complications often affect quality of life permanently.
3. Microvascular Decompression (MVD — The Open Surgery)
MVD involves a craniotomy (opening the skull) to separate a blood vessel that is compressing the trigeminal nerve root. While it can provide lasting relief for patients with confirmed vascular compression, it works only for neurovascular conflict cases — not for idiopathic or secondary trigeminal neuralgia. As a major neurosurgical procedure under general anesthesia, it carries the inherent risks of craniotomy, including infection, cerebrospinal fluid leak, stroke, and hearing loss.
💡 The Treatment Gap
Many patients — especially the elderly, those with multiple comorbidities, or those for whom medication has failed — find themselves trapped between insufficient medication and unacceptable surgical risk. This is precisely where Gamma Knife radiosurgery bridges the gap.
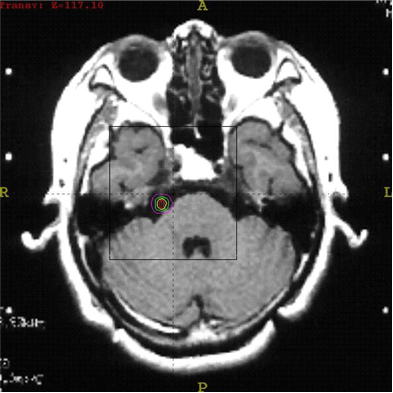
Pre-treatment MRI imaging is essential for identifying the target point on the trigeminal nerve. The precision of Gamma Knife radiosurgery depends on accurate localization through stereotactic MRI guidance.
4. Gamma Knife Radiosurgery (Non-Invasive Precision)
Gamma Knife treatment represents a fundamentally different approach. Instead of cutting or destroying large sections of the nerve, it delivers precisely focused beams of gamma radiation to a specific point on the trigeminal nerve root, selectively disrupting pain-conducting fibers while preserving touch and motor function.
The science behind this selectivity lies in the biology of nerve fibers. The trigeminal nerve contains different types of nerve fibers, each with varying sensitivity to radiation:
- Aδ fibers (pain and temperature) — the thinnest diameter and thinnest myelin sheath, most radiosensitive
- Aβ fibers (light touch) — thicker myelin, more radiation-resistant
- Motor fibers (mastication muscles) — thickest, most radiation-resistant
This biological difference allows Gamma Knife to achieve what surgery cannot: selective pain relief without collateral damage to touch sensation or motor function.
A Brief History: From Leksell to Today
The concept of treating trigeminal neuralgia with radiation dates back to 1953, when Swedish neurosurgeon Professor Lars Leksell performed the world's first stereotactic radiosurgery on two trigeminal neuralgia patients using orthovoltage X-rays directed at the trigeminal ganglion. Both patients experienced varying degrees of pain relief — an observation that would eventually lead to one of the most elegant solutions in functional neurosurgery.
With the invention of the first Gamma Knife in 1967 and subsequent advances in computer technology and medical imaging, Gamma Knife has evolved into a fully digitized, automated, and intelligent treatment system. Using multiple cobalt-60 sources precisely focused on a stereotactic target, Gamma Knife achieves sub-millimeter accuracy — a level of precision unmatched by any other radiation delivery platform.

The Gamma Knife radiosurgery system uses multiple cobalt-60 sources focused with sub-millimeter accuracy on the trigeminal nerve root, delivering a single high dose of radiation to block pain signals while sparing surrounding healthy tissue.
Clinical Efficacy: What the Data Shows
Gamma Knife radiosurgery for trigeminal neuralgia is supported by decades of clinical research and real-world experience. The evidence is compelling:
According to the landmark study published in the International Journal of Radiation Oncology • Biology • Physics (2011), which followed 556 patients over a median of 10 years, Gamma Knife radiosurgery provides durable pain relief with an excellent safety profile.
"The most important advantage of Gamma Knife treatment is that it enables patients to avoid craniotomy and the associated risks of general anesthesia, while still achieving meaningful and lasting pain relief."
It is important to note that results are not immediate. The onset of pain relief varies individually — some patients experience relief within hours, while others may take up to a year. However, the majority of patients (3 weeks to 3 months) begin to notice improvements within this window. During this waiting period, patients can continue taking their prescribed medications until the treatment takes full effect.
The Gamma Knife Treatment Process at GCCC
The entire procedure, from frame placement to completion, takes approximately 3 to 4 hours and involves five well-established steps:
- Stereotactic Frame Placement — A lightweight stereotactic head frame is secured to the patient's skull under local anesthesia, providing a fixed reference coordinate system for sub-millimeter targeting.
- MRI Localization Scan — High-resolution magnetic resonance imaging is performed with the frame in place to precisely identify the trigeminal nerve root target.
- Treatment Planning — A team of neurosurgeons, radiation oncologists, and medical physicists collaboratively design a personalized dose plan, determining the exact radiation dose and target configuration for optimal results.
- Treatment Delivery — The patient lies on the treatment couch while the Gamma Knife system automatically positions and delivers the radiation dose. The entire process is monitored in real time.
- Frame Removal — After treatment, the stereotactic frame is removed and the small pin sites are bandaged. Patients can typically resume normal activities within 24 hours.
Safety Profile and Side Effects
Gamma Knife radiosurgery has a well-characterized and generally favorable safety profile. The most notable potential side effect is mild facial numbness on the treated side, which occurs in a minority of patients. In most cases, this sensory change:
- Is mild and does not significantly impact daily life
- Tends to diminish or resolve over time
- Is generally considered an acceptable trade-off for freedom from debilitating pain
In rare instances, more persistent numbness or corneal complications (keratitis) may occur. However, modern dose optimization techniques have dramatically reduced the incidence of severe side effects. Most patients report the treatment experience as comfortable, with some transient dizziness or nausea largely attributable to pre-procedural anxiety rather than the treatment itself.
Who Is an Ideal Candidate?
Gamma Knife radiosurgery is particularly well-suited for:
- Elderly patients or those with significant comorbidities who cannot safely undergo craniotomy
- Patients with medication-resistant pain who cannot tolerate escalating drug doses or side effects
- Patients with idiopathic trigeminal neuralgia (no clear vascular compression on imaging)
- Patients with recurrent pain after previous surgical interventions
- Patients with bilateral trigeminal neuralgia or multiple sclerosis-related TN
It is essential that patients undergo comprehensive evaluation — including high-resolution MRI — to exclude secondary causes such as tumors or multiple sclerosis before proceeding with treatment.
After Treatment: What to Expect
Recovery after Gamma Knife is notably straightforward compared to open surgery. There is no hospital stay required for the radiosurgery itself, and patients should:
- Maintain a regular sleep schedule and prioritize rest
- Avoid or minimize known pain triggers during the onset period
- Continue prescribed medications as needed until the treatment effect fully manifests
- Attend scheduled follow-up appointments for monitoring
If pain persists during the onset period, patients may continue medications or receive local nerve blocks for temporary relief until the Gamma Knife effect becomes established.
🌟 Consult a Gamma Knife Specialist at GCCC
Whether you are considering Gamma Knife for trigeminal neuralgia or exploring treatment options for a loved one, our multidisciplinary team of neurosurgeons and radiation oncologists is ready to provide a personalized assessment.
Request a ConsultationAuthor: Dr. Liu Qiyong | Reviewed by: Prof. Qian Chaonan | Published by: Guangzhou Concord Cancer Center, April 17, 2026
Supported by: China Anti-Cancer Association (CACA) — Clinical Training Base for Integrated Oncology, Cancer Prevention & Screening Training Base, and Clinical Research Transformation Base